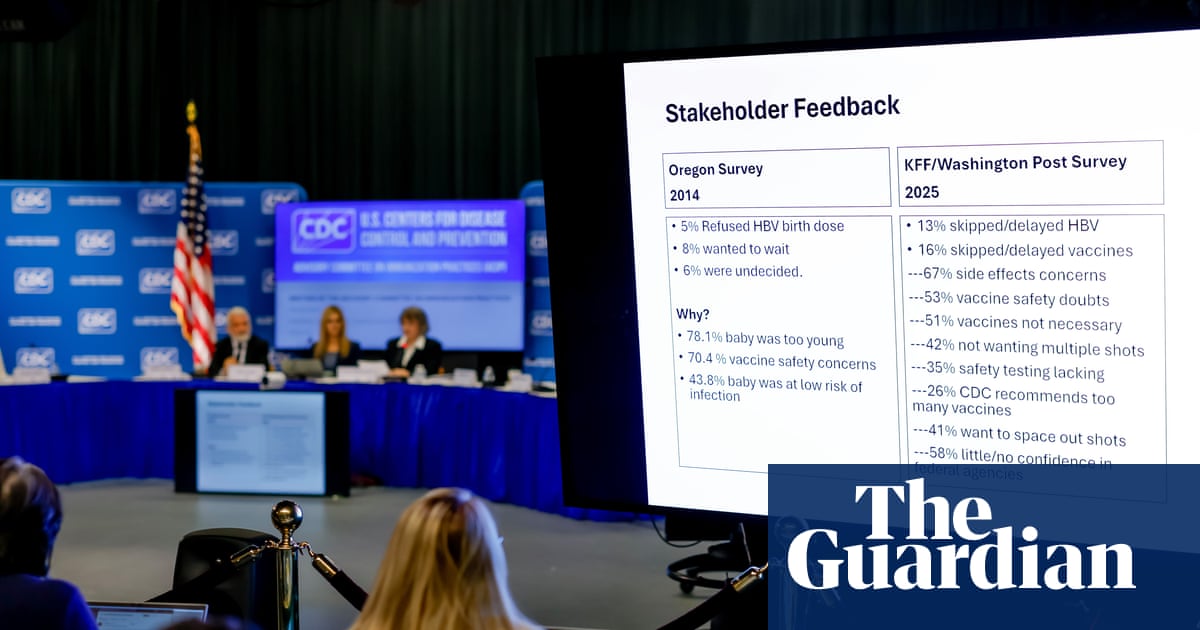
CDC advisory committee members, in a contentious session marked by leadership changes and the influence of anti-vaccine appointees, voted 6-3 to delay until Friday a decision on restricting universal newborn hepatitis B vaccination. The vaccine, given to roughly 1.4 billion people over decades, faced no new safety evidence, while researchers warned that delaying the birth dose to two months could cause ~1,400 infections, 300 liver cancers, 480 deaths and an incremental ~$222m in annual healthcare costs. The dispute and panel reshuffling introduce policy uncertainty that could erode public confidence in established childhood immunization schedules.
Market structure: Immediate winners are large, diversified pharma/vaccine makers (Pfizer PFE, Merck MRK, GSK) that can absorb reputational noise and benefit from any federal mitigation funding; losers are small-cap, pediatric-vaccine–dependent names (e.g., Dynavax DVAX) and niche contract manufacturers whose revenue is concentrated in routine infant immunizations. Competitive dynamics shift modestly toward incumbents with broad product portfolios and public‑health contract relationships; niche players face pricing pressure and volume risk if neonatal schedules are changed. Supply/demand: demand for neonatal hepB shots could fall near-term (weeks) if policy changes or public debate persist, but catch‑up demand and public campaigns could re‑accelerate volumes over 6–24 months, making the shock temporary. Risk assessment: Tail risks include a policy cascade that reclassifies routine pediatric vaccines into “shared clinical decision‑making” nationally (low probability, high impact) and state‑level litigation or mandates that fragment the market; loss of US measles eradication could trigger emergency funding or litigation. Time horizons: immediate (days) — acute volatility around the ACIP vote Friday; short (1–3 months) — pricing/volume repricing for small vaccine names and media-driven demand shifts; long (1–3 years) — potential sustained lower childhood-vaccine uptake, higher outbreak frequency, and political/regulatory oscillation. Hidden dependencies include state school‑entry mandates, CDC messaging budget, and pharma contract timelines that can blunt or amplify revenue shocks. Trade implications: Favor defensive, cash‑generative large pharmas (PFE, MRK) and reduce exposure to pure‑play vaccine small caps (DVAX) with explicit size limits and event triggers. Use pair trades (long MRK or PFE, short DVAX) to isolate policy risk and buy protective puts on small caps rather than outright shorts to limit tail losses. Entry should be staged: small initial positions ahead of the Friday vote (within 48–72 hours), increase only if the ACIP signal turns adverse; exit or tighten stops within 7 trading days after a clear CDC ruling or federal corrective action. Contrarian angles: Consensus underestimates two outcomes: (1) a policy change may be reversed rapidly under public‑health and legal pressure, creating a short squeeze in beaten‑down small caps; (2) federal remediation (campaigns/funding) would favor large makers and vendors (ad tech, public‑health contractors). Historical parallels (measles scares 2019) show big pharma earnings were resilient; therefore avoid over‑hedging legacy pharma exposure. Set hard triggers: if CDC votes to delay to 2 months, increase small‑cap shorts to target sizes; if vote preserves birth dosing, cover shorts within 5–7 days to capture mean reversion.
AI-powered research, real-time alerts, and portfolio analytics for institutional investors.
Request a DemoOverall Sentiment
moderately negative
Sentiment Score
-0.30