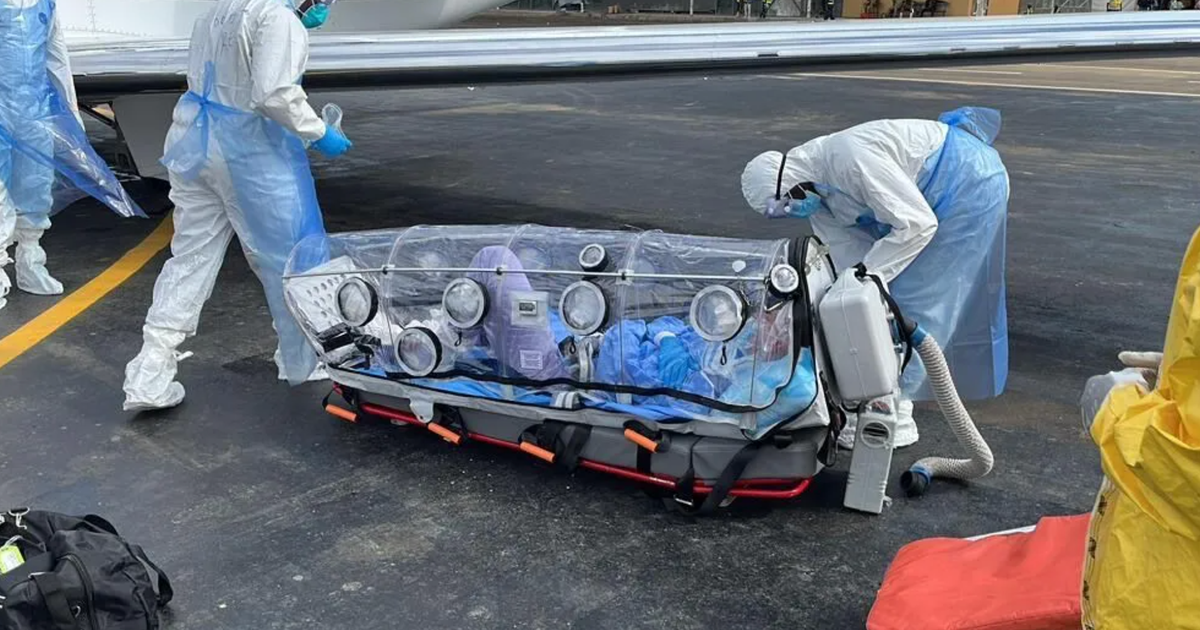
An American doctor infected with Ebola in the Democratic Republic of Congo was evacuated to Berlin and is described as critically ill but not acutely deteriorating, while his wife and four children were also evacuated and remain asymptomatic. The outbreak involving the Bundibugyo strain is now reported at nearly 600 suspected cases and 139 suspected deaths, with officials warning it may be larger than officially reported. The U.S. has also imposed airport entry restrictions for recent travelers from Congo, Uganda and South Sudan.
This is a classic localized-health-event becoming a broader policy and logistics shock rather than a direct market-wide growth shock. The near-term winners are not vaccine makers here — there is no direct tradable prophylaxis angle for this strain — but rather the infrastructure that gets paid when governments and NGOs rush to harden screening, isolation, medevac, and biosafety protocols: airport screening vendors, PPE/logistics suppliers, and select hospital service contractors. The second-order effect is that any outbreak-linked travel restriction reinforces the premium on firms with Africa exposure and complex cross-border operations, particularly where staffing continuity is already fragile. For healthcare, the bigger issue is operational drag. Hospitals and missionary-linked care networks in frontier markets face higher labor turnover, higher insurance costs, and a slower willingness of expat clinicians to deploy, which can suppress elective and surgical throughput for months. If the outbreak is indeed undercounted, the market’s error is likely in underestimating duration rather than severity: containment can happen quickly, but reputation damage and travel friction persist well after case counts stabilize. The geopolitical read is that this increases scrutiny on East/Central African mobility and can tighten visa, quarantine, and evacuation protocols in a way that raises transaction costs for NGOs, mining, and logistics operators in the region. That matters for broader EM risk appetite at the margin: not because of direct revenue exposure, but because investors tend to reprice frontier-risk premia upward whenever medical containment appears weak. The contrarian view is that the selloff/avoidance impulse may be overdone for global healthcare names; absent a vaccine/treatment race, the event is more about services and compliance spend than large-cap therapeutics. Time horizon matters: the next 1-3 weeks are about policy headlines and airport/travel controls; the next 1-3 months are about whether cases spread beyond localized clusters and force broader mobility restrictions. A clean containment path would unwind most of the risk premium quickly, but a prolonged surveillance campaign keeps a bid under biosafety and remote-care themes.
AI-powered research, real-time alerts, and portfolio analytics for institutional investors.
Request DemoOverall Sentiment
strongly negative
Sentiment Score
-0.65